
Standing and walking are self-evident until … .. until, for whatever reason, people are not able to anymore. Then what? Find a doctor or therapist for help. But what, if they do not find it?

For (chronic) postural complaints such as (low)back-, foot-, shoulder- and neck pain, there might be still a solution:
This specialty is known as podopostural therapy.
This site is meant to:
- to give (chronic) patients a perspective
- to help them analyze the (possible) causes and communicate them intelligibly. Preferably in consultation with other disciplines. Years of observation convinced me that the only way to look at human posture is 3-D !! In the early nineties I introduced my 3-D posture scheme:
Posture Quadrant Theory
With my book Regulation therapy from the foot (Regulatietherapie vanuit de voet, Peter Oomens, Tijdstroom, 1991) I have introduced the posture quadrant theory.
‘Podo professionals’ talk about the same foot, often from a different point of view. Podiatrists, physical therapists, physicians, Shiatsu therapists, they all have their own theories how to examine and treat podologic disorders.
Foot reflexologists sometimes claim results which do not seem realistic from a neurophysiological point of view.
As a posturologist I have treated patients with postural disorders, often by podologic intervention. Based on the ideas of Dr René Jacques Bourdiol I came more and more to the conclusion that his therapy has proven and proves to be effective, but that his theory behind it raises questions:
- It is hard to believe that pieces of cork or whatever material at a thickness 1- 2 mm can influence the intrafusal γ-fibers through dermis, epidermis, plantar tissue and ligaments.
- Bourdiol discussed the foot and the human posture in a two-dimensional way.
Although still theoretic it is, with my publication in 1989, my suggestion that the obvious effect of the so called Bourdiol proprioceptive insoles, is obtained by influencing the mechanoreceptors of the glabrous skin of the foot sole. Only when under pressure during stance and gait. In fact we are talking about ‘exteroceptive’ therapy soles. Today’s literature also points in this direction.
Balance a moment only on both heels. Not really comfortable. Yet on the toes: same conclusion.
We stand on four ‘balance points’ with our body ‘swaying’ in between. Not only frontal and horizontal, but also sagittal. The more close to the optimal body’s gravity point, the less muscle activity is required.
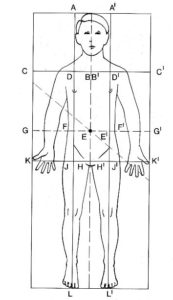
My quadrant theory now is based on:
1. The body struggles against gravity. Considering that originally we were a biped, we tend to ‘fall’ forward. So our struggle against gravity is backward.
2. Each change of a local gravity point (arm for example) lead to a compensatory reaction elsewhere and always affects the position of the general body gravity point.
3. A mirrored reaction takes place from L 3. A correction above L 3 is corrected under L 3, always influencing the general body gravity point
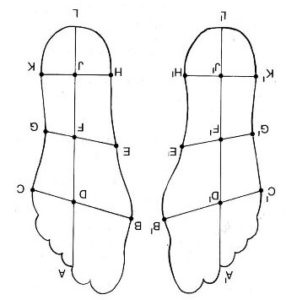
The subdivision of the plantar foot in my scheme is corresponding with the body ’s subdivision. Increased pressure on a particular spot under the foot is related to a particular body part.